


Diagram courtesy of ConvaTec Canada
What's a stoma and how’s it made?
Many of you were pretty sick before ostomy surgery. Researching what a stoma is, how it's made and what it's made of may have been the least of your concerns. Interestingly, the word stoma comes from the Greek meaning a mouth or opening. You, the patient, provided the material - aren't you glad you were able to help?
Both the words "stoma" and "ostomy" mean the same thing. An opening in made in your belly wall and a portion of your large bowel or a portion of your small intestine is brought through the opening. After the stoma is bought through it is folded back and it is then sutured to the skin. Depending of the type of ostomy surgery, the stoma is attached to the left or right side of your stomach. Stool or urine can now leave the body after it became difficult or impossible to do so in the normal way.
The Digestive Tract
Sometime, before or after your surgery, you may start to be curious about exactly what happens to your food after it passes your lips. The second link below is worth a visit
Resources
ConvaTec Canada How is a stoma surgically created
Blausen Medical Communications The Components of the Digestive System
Colostomy
The most common reasons for requiring colostomy surgery are cancer of the colon, diverticulitis and trauma. Colostomy surgery will result in some part of your colon being brought out of your abdomen.

Descending Colostomy
A more common type of colostomy. Output is semi-formed to formed due to more water being absorbed while in the ascending and transverse colon.

Transverse Colostomy
Output is liquid to semi-formed. Usually constructed as a loop. Usually temporary.

Ascending Colostomy
Uncommon type of colostomy. Output is liquid to semi-liquid and very irritating to the skin.
The detailed diagrams & text following show the placement of stomas when the procedure is expected to be reversed and are used with permission from the Nurses Specialized in Wound, Ostomy and Continence Canada (NSWOCC)

End Colostomy
An end colostomy is usually located in the lower left colon (sigmoid). If the anus, rectum and part of the lower colon have been removed, this type of colostomy is permanent (Diagram #2).

End Colostomy With a Mucous Fistula
If the anus, rectum and a portion of the lower colon have not been removed, two stomas may be created. One stoma leads to the functioning part of the colon through which stool and gas pass. The second stoma opens into the non-functioning portion of the colon and rectum and is called a mucous fistula (Diagram #3). The second stoma is usually small, flat, pinkish-red in colour, moist and produces only mucus. When the rectum remains in place, the urge to have a bowel movement may occur, but only mucus and possibly some old stool, if present, will be passed.

End Colostomy With a Rectal Stump
Sometimes the end of the lower non-functioning part of the colon and the rectum is stapled or sewn closed and left inside the abdomen. This piece of bowel left inside is called a rectal stump (Diagram #4). If the colostomy is temporary, once healing from the first surgery is complete, a second surgery is required to reconnect the two ends of the bowel.

Loop Colostomy
A loop colostomy is most commonly created if the colon is blocked. This type of colostomy is also used to divert stool from a diseased, injured or healing colon. The stoma site is usually located high on the abdomen above the waistline. If the colon was blocked, the stoma may be very large immediately after surgery but usually shrinks as the blockage is relieved and healing occurs. A loop colostomy may be temporary or permanent and has two openings. One opening leads to the functioning part of the colon through which stool and gas pass. The second opening leads to the non-functioning part of the colon and allows mucus and old stool, if present, to pass from the rectum through the anus (Diagram #5).
Resources
An excellent "everything"guide: Colostomy Guide
ConvaTec Canada: The Basics Colostomy Surgery
Hollister Canada: Ostomy Educational Theatre - Colostomy
Hollister: Ostomy Care Resources
United Ostomy Association of America: Being a teenage colostomist
Coloplast: Understand Your Stoma Surgery
UOAA: Living with a Colostomy
UOAA: Irrigation FAQ's
UOAA: Irrigation Guide
UOAA: Sexuality
Ileostomy
The most common reasons for requiring Ileostomy surgery are Ulcerative Colitis, Chrohn's disease, Cancer complications, familial Polyposis (an inherited condition) and trauma. Ileostomy surgery will result in most, if not all, of your large bowel (colon) being removed. The ileum or end of the small bowel, is brought out and becomes your stoma.

Diagram noted as being in the Public Domain

Diagram & Text courtesy ConvaTec Canada
The end Ileostomy is located in the ileum which contains digestive enzymes and acids that may cause skin irritation. Extra care is needed with an ileostomy to keep waste materials from coming into contact with the skin on your abdomen.
Having an ileostomy may make some people more prone to dehydration, which could lead to the loss of important minerals your body needs.

Canadian Association of Enterstomal Therapy (CAET), 2015
A loop ileostomy may be created to divert stool from diseased, injured or healing bowel. It is usually temporary and has two openings. One opening leads to the functioning part of the small intestine through which the drainage and gas pass. The second opening leads to the non-functioning part of the small intestine and allows mucus and old stool, if present, to pass from the rectum through the anus.
Resources
An excellent "everything" Guide: Living with an Ileostomy
Ostomy Canada: A Guide to Lving with an Ileostomy
Ostomy Care Canada: Understanding Your Ileostomy
Coloplast: Understanding Your Stoma Surgery
Alberta Health Services: Eating Well After Ileostomy Surgery
NHS UK: Recovering and Lifestyle after an Ileostomy
Stoma Tips: How I got my Stoma at 16
Urostomy
Urostomy surgery becomes necessary when the bladder stops working properly. There are many reasons; a few are because of bladder cancer, a spinal cord injury or a birth defect.
Urine is waste produced from your blood due to the filtering function performed by your kidneys. Everything that is left over after purification such as salts, urea, toxins and surplus water becomes urine that moves down to your bladder. Peeing removes these wastes.
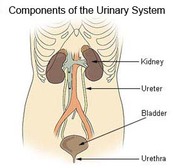
Image courtesy of US Dep't of Health SEER Urinary System

Diagrams & text both above and below used with permission from the Canadian Association of Enterstomal Therapy (CAET), 2015
The urinary tract consists of two kidneys, two ureters, one bladder and one urethra (Diagram #1). Urine is made in the kidneys and flows through the ureters into the bladder, where it is stored. The bladder is a soft balloon-type organ that stretches as urine fills it and contracts when it is emptied. The urethra is the tube that drains urine from the bladder to the outside of the body.
A urostomy is a surgically created opening to divert urine from its normal route. This surgery is necessary when the bladder must be removed or bypassed. Children who have urinary tract birth defects may need a temporary urostomy.
Urostomies are usually permanent for adults. Common reasons for performing urostomies in adults include: cancer of the bladder, spinal cord injury resulting in loss of bladder control, and neuromuscular diseases such as multiple sclerosis.
The most common type of urostomy is called an ileal conduit. To create the conduit, the surgeon isolates a short piece (about 10 cm) of small intestine (bowel) (Diagram #2). The small intestine is reconnected and functions normally.
The piece of isolated bowel is closed at one end. The other end is brought to the outside of the abdomen, turned back on itself like a cuff of a sleeve creating the stoma and sewn to the skin. The ureters from the kidneys are attached into this piece of small bowel, which is now called the conduit (Diagram #3).
The part of the small intestine known as the ileum is used to make the conduit; therefore, the urostomy is called an ileal conduit (Diagrams #2 and #3). The urine is excreted from the kidneys and drains through the ureters into the conduit. From the conduit the urine drains through the stoma. The ileal conduit is not a storage cavity and urine drains most of the time. A pouch must be worn at all times to collect the urine.
Cecostomy
A cecostomy is a tube placed into the body near the Cecum, at the beginning of the large intestine. There is an exterior component and an interior component. The tube is used to assist in evacuating the bowels of stool/poop and for maintaining continence during the day. Typically, it is placed when there is no disease in the bowel, but the body can not achieve continence. For a MACE, the tube stays in the body and is not removed. For a Chait or Mic-Key tube, it needs to be changed with a new tube on a basis provided by the doctor, but otherwise does not come out.
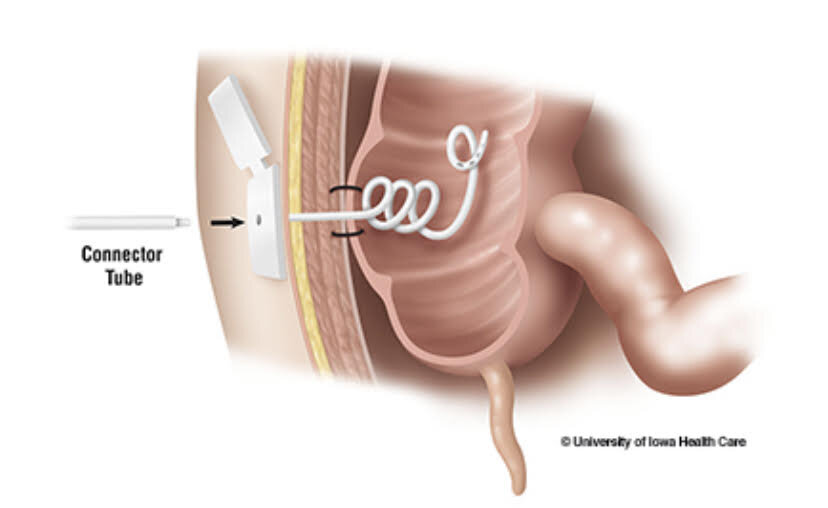
Chait
Once the cecostomy is placed and the site is healed, the person will irrigate the bowel using the tube. This may be called a “flush” or a “routine”. An enema/laxative is brought to the bowel via the cecostomy and extensions added. The doctor will go through the particular substances and measurements, as well as length of the routine, at some point during the initial implantation.
Most common reasons for getting a cecostomy are Spina Bifida, the person is born with an imperforate anus, and other muscular abnormalities.
There are two main types. A MACE, also called a Malone, has a “bubble” at the end of the interior portion of the tube. It is slightly larger than a chait. A Chait has a trapdoor device on the exterior and a curled tube inside.
Resources
An excellent “everything” guide: A Guide to Living with an Ileal Conduit
ConvaTec Canada The basics - Urostomy Surgery (Excellent illustration and description of an ileal coduit)
Coloplast – What is a Urostomy
Coloplast: Urostomy Guide to Living Well
The UK Urostomy Association
Ostomy Care Canada: Understanding Your Urostomy
UOAA: Living with a Urostomy
Coloplast: Life after Urostomy
Bladder & Bowel Community: How Having a Urostomy Improved My Life
American College of Surgeons - Emptying your Urostomy Pouch
https://www.youtube.com/watch?v=0o55KfNNw2w
American College of Surgeons - Changing your Urostomy Pouch
https://www.youtube.com/watch?v=qRmUOlCgigg

MACE